
Gallstone disease is considered a benign disease affecting large amount of population. The number of patients with gall bladder diseases is on rise. It demands major abdominal surgery. Among various diseases [1]. Cholelithiasis, or gallstones is most common one. It is evident in literature that the occurrence of gallstones increases with age [2]. Risk factors includes obesity, diabetes mellitus (DM), women gender, rapid weight cyclers, and patients on hormone therapy or taking oral contraceptives. Until and unless, gall stones pose pain, they remain asymptomatic [3]. Most of the symptomatic patients shows symptoms of biliary colic due to the intermittent obstruction of the cystic duct by a stone. Patient experience moderate to severe pain which lasts one to five hours. Pain is usually localized to the epigastrium or right upper quadrant of the abdomen [4].
The occurrence of fever along with colic pain with high white blood cell count (WBCs) raises the suspicion of complications such as acute cholecystitis, gallstone pancreatitis, and ascending cholangitis [5]. The diagnosis of gall stones is by ultrasonography (USG). USG is useful in detection of gall stones [6].
The management of cases of gall stones includes laparoscopic cholecystectomy. It is gold standard treatment options for symptomatic and complicated gallstones [7]. Advantages of this modality is shorter convalescence period and short hospital stay comparing to open cholecystectomy [8]. Percutaneous cholecystostomy is an alternative for patients who are critically ill with gallbladder empyema and sepsis. It is found that adhesions are amongst the common reasons for open conversion of laparoscopic cholecystectomy [9]. We attempted this study to compare single versus multiple gall stone disease in patients undergoing laparoscopic cholecystectomy.
All were those who gave their consent for the part of this study. Randomization of them into 2 groups was performed. Group 1 comprised of single stone patients and group II had multiple stones. A routine laboratory investigation comprised of Hemoglobin % (Hb), total leucocyte count (TLC), differential leucocyte count (DLC), random blood sugar (RBS), serum urea and creatinine was carried out. Apart from this, Assessment of serum bilirubin, serum amylase, alkaline phosphate, bilirubin total, renal and liver function test was determined. Before operating the patients, electrocardiography (ECG) and chest X-ray (CXR) were performed.
Advanced imaging such as ultrasonography of abdomen (USG) was done to study the nature, number, size of the gall stones, gall bladder wall thickness, CBD, intra hepatic biliary radicals status, any other relevant findings. Computed tomography (CT) scan and magnetic resonance imaging (MRI) was carried as and when required. Results after recording all relevant data were subjected for statistical inferences using chi- square test. The level of significance was significant if p value is below 0.05.
Maximum cases were seen in age group 40-50 years in both groups (group 1- males- 16, females- 20, group 2- males- 15, females- 20). Minimum cases were seen in age group 20-30 years (group 1- males- 5, females- 6, group 2- males- 2, females- 5). A non- significant in gender was observed \((P> 0.05)\), see Table 1.
| Age group (Years) | Group 1 (M:F) | Group 2 (M:F) | P value |
|---|---|---|---|
| 20-30 | 5:6 | 2:5 | >0.05 |
| 30-40 | 2:10 | 5:6 | |
| 40-50 | 16:20 | 15:20 | |
| 50-65 | 4:8 | 3:3 |
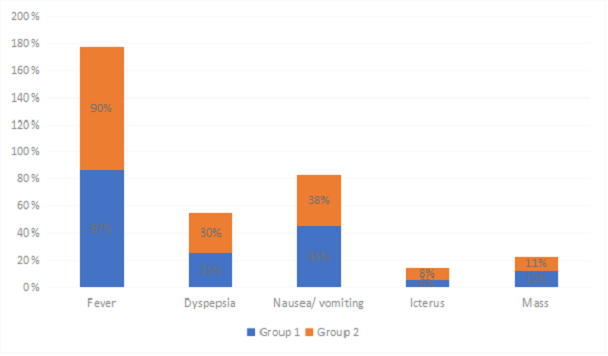
Most common clinical symptoms found to be fever in both groups (87%- group 1, 90%- group 2). Other symptoms were dyspepsia seen in 25% and 30%, nausea/ vomiting in 45% and 38% in group 1 and 2 patients respectively. A non- significant in gender was observed \((P> 0.05)\). (Table 2, Figure 1).
| Clinical findings | Group 1 | Group 2 | P value |
|---|---|---|---|
| Fever | 87% | 90% | >0.05 |
| Dyspepsia | 25% | 30% | |
| Nausea/ vomiting | 45% | 38% | |
| Icterus | 6% | 8% | |
| Mass | 12% | 11% |
Group 1 patients showed gall bladder distention in 56 and group 2 in 62 patients, gall bladder contraction was seen in 6 patients in group 1 and 3 in group 2, adhesions were exhibited by 11 patients in group 1 and 20 in group 2. 4 patients in group 2 converted to open surgery. Gangrenous gall bladder was seen in 1 in group 1 and 5 in group 2. A significant difference was observed \((P< 0.05)\), see Table 3.
| Operative findings | Group 1 | Group 2 | P value |
|---|---|---|---|
| Gall bladder distension | 56 | 62 | < 0.05, Significant |
| Gall bladder contraction | 6 | 3 | |
| Adhesion | 11 | 20 | |
| Gangrenous gall bladder | 1 | 5 | |
| Conversion to open surgery | 0 | 4 |
Our study comprised of 130 patients divided into 2 groups of 65 each based on the presence of single or multiple stones. It was found in our study that maximum cases were seen in age group 40-50 years in both groups (group 1- males- 16, females- 20, group 2- males- 15, females- 20). Minimum cases were seen in age group 20-30 years (group 1- males- 5, females- 6, group 2- males- 2, females- 5). Mofti et al., [16] evaluate 692 consecutive patients undergoing cholecystectomy of whom 80 had single stone. Only about 30% asymptomatic patients need surgery in their life-time.
It was observed that most common clinical symptoms were fever in both groups seen among 87% in group 1 and 90% in group 2 patients. Other symptoms were dyspepsia seen in 25% and 30%, nausea/ vomiting in 45% and 38% in group 1 and 2 patients respectively. A study by Zhang et al., [17] suggested that LC is the gold standard in the treatment for cholelithiasis. Prophylactic cholecystectomy is justified only high suspicion of life. They found that developing mucocele, empyema gall bladder perforation and post-operative complication were more common in patients with solitary stone. Gabriel et al., [18] in their study observed that 61 (26.1%) LC required conversion.
It was seen in our study that 56 patients in group 1 and 62 in group 2 showed gall bladder distention, gall bladder contraction was seen in 6 patients in group 1 and 3 in group 2, adhesions were exhibited by 11 patients in group 1 and 20 in group 2. 4 patients in group 2 converted to open surgery. Gangrenous gall bladder was seen in 1 in group 1 and 5 in group 2. A study conducted by Raja et al., [19] in year 2020 where patients of gall bladder stones were divided into 2 groups as single or multiple stones. In both groups, female incidence, 41-50 years age group is more common. Both groups presented with abdominal tenderness (RUQ), fever more in group-1, dyspepsia more in group-2 and icterus more in group-2. Complications of gall stones as suggested by USG of abdomen like cholecystitis, gangrenous cholecystitis, gallbladder perforation, empyema of gallbladder were more in multiple than single stone patients. Group II had difficult cholecystectomies based on the above timings noted intraoperatively.
The natural course of gallstone disease is benign, with relatively low progression from asymptomatic disease to symptomatic disease. Natural history studies have shown low mortality from gallstone disease with typically less than 1% of people dying from gallbladder-related causes. Festi et al., study (2010) [20] revealed that the overall frequency of symptom development in asymptomatic people was around 20% over a long follow-up period (mean 8.7 years). In people with symptomatic uncomplicated gallstone disease, the annual rates of developing complications have been reported to be as low as 1%-3%. The Italian Group for the Epidemiology and Prevention of Cholelithiasis Study reported an annual incidence of complications of 0.7% for symptomatic people.